
In a couple of hundred words on the last Friday before Christmas, a short piece talked about what the recent HDR/Sudlow Review means for you and how the Government thinks it will use your medical history and your medical notes in ways you may not entirely like. This blog post is a little longer than that – we look at what they’re already doing and how.
Wes Streeting wrote that patients should be given weight loss drugs because they’re “holding back our economy”. Afterwards, he went into damage control mode. His original quote cut through so far that his response saying “Jabbing unemployed people who are overweight – that is not the agenda” has made it into the BBC Newscast podcast opening credits. Jabbing unemployed people who are overweight is exactly what he announced. Streeting doesn’t want to be dystopian, but perhaps the important thing is the outcome not his personal intent.
The Treasury’s instruction to Departments was “stop non-priority spending” and then the Department of Health in England then gladly put out press release how they were complying:
“NHS England is working with the Office for National Statistics to assess the economic benefits of several health interventions including talking therapies, bariatric surgery, treatment for endometriosis, and the NHS Type 2 Diabetes Prevention Programme.
The analysis will also cover the impact on waiting times, employment rates and earnings while feeding into work by the Office for Budget Responsibility and the government on labour market effects.”
DH/E and HMT refuse to say whether the instruction to prioritise public funds for economic growth, and the instruction “not doing things” that don’t grow the economy, apply to the NHS. NHS England clearly thinks they do. When reviewing the project, NHS England’s Independent Advisory Group on Data (AGD) asked if HM Treasury should be named as a joint data controller for this project (section 5.1.10). In order to prioritise treatments that assist the economy in a fixed NHS budget, the Government will also have to deprioritise treatments that help patients but don’t measure as helping the economy.
Your health records linked to your tax records is how that is measured, and they’ve already started. The HDR/Sudlow Review covers their perspective on how that should be done and what the Office of National Statistics should do with data. ONS convened the review because ONS has a major problem – they culturally insist they have the support of the public for what they do with data, but they measure that support by response rates to their surveys, and public support has collapsed to only 20% and falling.
In response, like other abusers of power who want to feel they were thinking like Obi Wan, ONS found it easiest to act like Vader.
The context: All your medical history and medical notes all in one place to be used however the Governments wants
The proposal for a Single Central Care Record has been announced and re-announced several times now as Wes Streeting’s “big idea” to help the NHS. It will put your entire medical history inside Palantir/FDP where DH/E can run AIs over it to do “population health management” and where access can be offered to your medical notes anywhere the NHS logo is seen – not just any doctor you see, but any doctor you could see (including private doctors and hospitals). Will any creepy single doctor anywhere in the NHS be able to look up your full medical history including all medical notes? Probably.
At this time we don’t know whether you will be forced to have one of these records, or what transparency will be around where your record is accessed. Given how DH/E are talking about the record, you are likely to be forced to have one as it is for direct care but it is replacing existing systems which do have an opt out, so who knows. The Department of Health in England has repeatedly sided with creeps over their victims.
When thinking what data the HDR/Sudlow Review covers, it is not just your hospital records, but all your GP records and all your written notes, and anything any other part of government (DWP, HMRC, DfE, etc) may know about you, all linked together and available to civil servants with no obligation to disclose what it’s used for unless someone in Parliament asks.
One argument made throughout is that data is only used for “public good”. There is a vast difference between what the Government of the day thinks of as “public good” and what is good for you. Austerity was a public good according to the Government of the day.
When a pregnant woman shares her heart rate readings 24/7 with her doctor for her health, it is the position of HDR/Sudlow that the Department of Health in England should be able to sell those data so they can be mined by anyone who pays the access fee. It is the position of DH/E that there is no opt out for you from the sale of that data – the choice is literally your data or your life…
HDR/Sudlow in brief: Clubcard Culture sends more data to more places more recklessly
As described on page 167, Biobank wants the Department of Health in England to reuse data that was collected with the promise of “pandemic only”, and give it away to Biobank and others to hand out like any other NHS data. Buried on pg 102 is the desire to collect and share data from your smartwatch and on pg 103 your loyalty card. In practice, that would be the NHS collecting your smartwatch and loyalty card transactions and placing them in Palantir for Biobank and others to copy and rifle through.
One slide from the launch sums it up – it shows Clubcard data and smart watch data being copied to the NHS and onwards to research and commercial use – but that slide doesn’t mention the very controversial HMRC tax data that ONS and NHS are using to change waiting list priorities. Funny that…
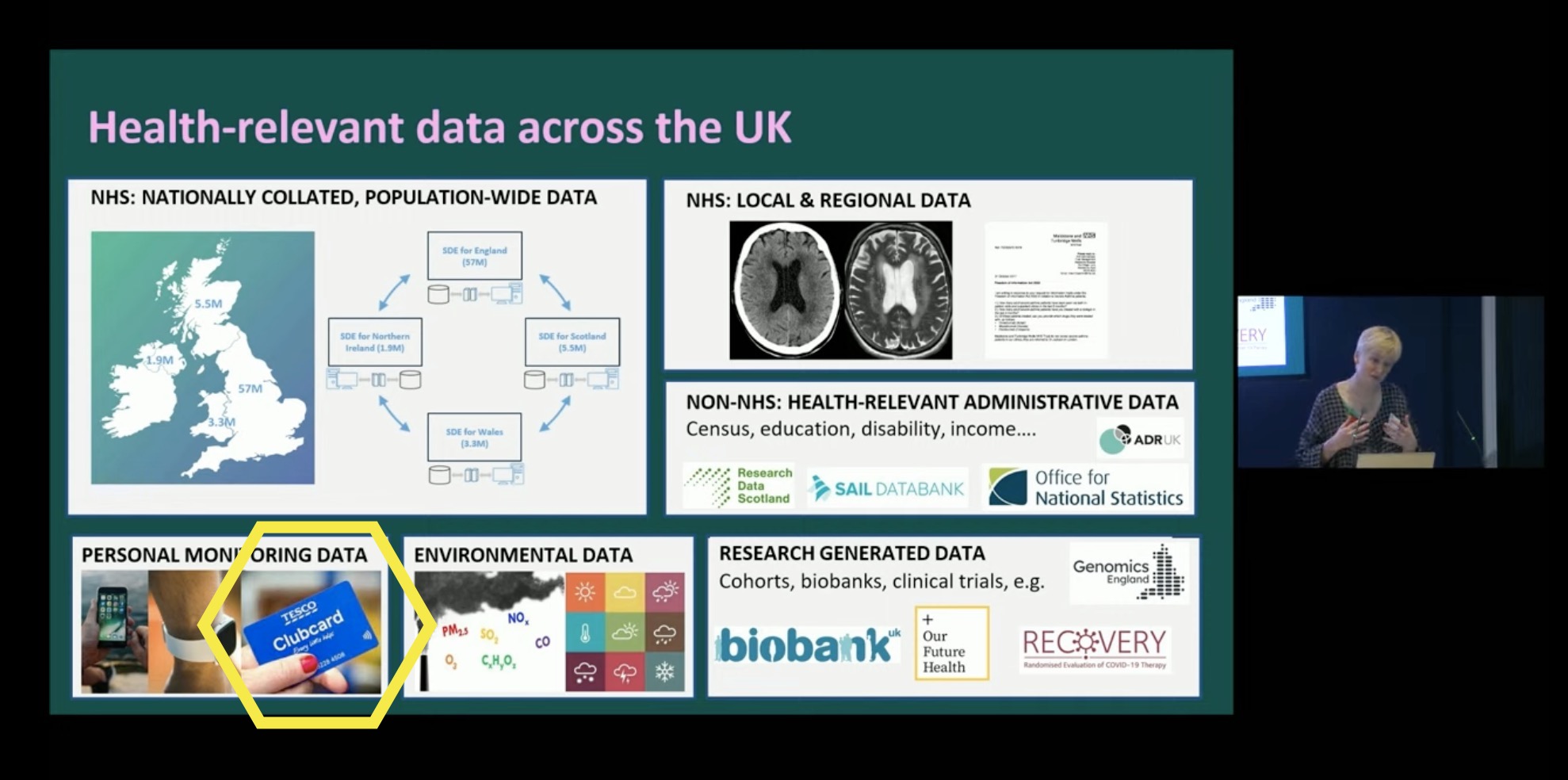
Recent research shows that the smartwatch on your write can help diagnose a range of conditions earlier, but that level of detail can also be used to
HDR/Sudlow: Biobank as the role model for more recklessness
Proposing that more data goes to Biobank to go to racists doesn’t grow the economy for everyone, it just grows some bank balances. Biobank believes that’s ok (still) because they pay Biobank’s fees.
Speaking at the launch, the report author said the goal was applicants getting data in “days” and proclaimed Biobank have “one of the best systems” for giving data out rapidly (without sufficient checks on who they gave it to).
We must note the Review author’s previous job from 2011-2019 which was getting more data for the disgraced regime at the UK Biobank during the period that the rules were watered down which meant Biobank handed the genetic data of the Biobank cohort to eugenicists, then moved to the mess that is HDR (the two organisations share a culture).
Biobank continue to angrily deny that people connected to the organisation Biobank gave data to, including the EIDs field, have access to the EIDs field that Biobank gave them (the full investigation)
The Department of Health in England are auditing Biobank, but it’s unclear whether that audit will cover Biobank processes which led to the coverage in 2024, or whether the audit will be narrow and restricted only to questions around insurer access by the Guardian in 2023, possibly also excluding the story from 2022 about Biobank selling data to China (nothing seems to be happening about our 2024 followup to that – Biobank ignored our questions). Biobank’s main concern seems to be whether they have received money from applicants, only checking that the applicant isn’t on Biobank’s list of known racists to reject – a list that will always be incomplete.
The NHS application form is 30 pages, the Biobank version is only three pages. Biobank continue to insist that nothing in those 27 pages matters (and nothing in their contract with NHS England requires them to ask anything in those pages), but the checks are so laxthat Biobank didn’t spot an applicant was a bunch of eugenicists operating out of the same fake office as QAnon sites and other scams. That’s the approach HDR/Sudlow and ONS wants to all public sector data.
Biobank repeatedly argues that eugenicists keep trying to get Biobank data, and when Biobank catches them they’ll say no (pity about the cases they’ve said yes to). Biobank claim not to understand the approach of making multiple requests until it works, yet Biobank keep repeating their demands that data they should get Biobank think they deserve without following the rules, and will keep stomping their little feet (and getting meetings with Ministers) until they get what they want – the ripping up of promises to patients.
HDR/Sudlow’s friends shouldn’t have to keep their promises?
Unless patients can see how data is used, the government will get lobbied to break every promise they’ve ever made to patients whenever the day ends in “y”, because no patient can tell the difference. This report is another example of that – HDR/Sudlow Review agrees with Sudlow’s previous lobbying job that their friends should get a free pass out of their obligations.
Following the Review’s recommendation, DH have announced that they’re going to give the “pandemic only” GP data to Biobank and others under terms that are not limited to the Covid19 but will be for whatever Biobank, Our Future Health (and others) think they can do usefully with the data in future (and only they get to decide that, no one else has a say)
HDR/Sudlow: only HDR’s Sockpuppets should be listened to
The Review says some things about consultation and engagement, picking winners from amongst consultation respondents by choosing those deemed a “good” consultee because they agree with what HDR/Sudlow wants to hear. HDR has form for this in designing an supposedly “open” call for applications in which UKRI will channel public funds to the “single collaborative bid” HDR chooses to support (the bid of their friends)
Unfortunately and embarrassingly for the authors, the HDR/Sudlow Review was so distracted by ensuring the Review only included the views of HDR that it forgot to suggest anyone else be invited to the group that supposedly should write the rules. The Review was so far in an echo chamber it forgot all it was listening to was itself.
According to HDR/Sudlow (pg 163), those that “would be well positioned to lead on SDE standards” is only “HDR UK [legal entity: HDR], ADR UK (partner with HDR but legally part of UKRI who fund HDR), the UK Health Data Research Alliance [legal entity: HDR], and UKRI’s Data and Analytics Research Environments UK (DARE UK) programme[legal entity: HDR]” and no one else. We have covered at length the ongoing subversion of safeguards by HDR as they continue their cash to cronies grants process and closed shop.
DH/E may be told they’re hearing from four organisations, but all bar one are sockpuppets controlled (in the data controller sense and in the practical sense) and owned by HDR where all the people in the room report up to HDR’s leader Andrew Morris and follow his party line.
Similarly, many of the public engagement groups of which HDR/Sudlow speaks supportively – PEDRI [legal entity: HDR], DAREUK [legal entity: HDR], etc are again simply HDR hiding behind another logo. The one exception (UseMyData) have staff funded by HDR and other staff paid by NHS England to do engagement work – entirely legitimate but difficult to be considered independent from HDR’s desires around NHS data.
Biobank and HDR want all data the NHS has, and they act as useful idiots for others who want that data for their own gain, including the Secretary of State who has an idea…
The Review was written to justify what was already being done
The NHS England announcement gives four examples where DH/E knows that there is a clear investment case to be made for funds, which is good for the bits of DH/E managing those waiting lists, but in a fixed budget imposed by HMT, that takes cash away from other treatments.
Focussing on economic benefits means “economic growth” supplants clinical decision making and prioritisation. The more say HMT has, and the more control the Department of Health in England takes, the less choice your doctors have.
The obesity work has already been done in the pilot, and now will be repeated with the other three areas (the work is being done by statisticians who like comparability). Ian Diamond talked about the work at the launch of the Sudlow Review where he disclosed that the existing work was done by ONS linking together taxpayer records with their health data, something the HDR/Sudlow review seems to have obfuscated in the Review itself.
All your health records and all your tax records linked, for departments to do with whatever they see fit. Once they’ve done these four areas, it is bureaucratically indefensible for not comparing all treatments across all of the NHS – what happens if there’s one that offers more benefit? But it will also show all treatments that have patient benefit but not measurable economic benefit. According to ONS (item 5.1 in April), the organisation making these decisions should be ONS, not the NHS. ONS makes decisions about the value of a statistical analysis, without any regard for the impact on patients or health.
ONS can do this because when NHS England gave them data for statistics purposes, NHS England chose not to respect the National Data Opt Out because it wasn’t identifiable data that would be linked onto your tax records (supposedly). Once ONS got the data for something, it can reuse it for anything. The NHS England Advisory Group on Data was not entirely happy (section 5.1 in October) but NHS England doesn’t appear to care.
Despite the use of tax records being discussed at the launch of the Sudlow Review, the diagram on page 123 of the report notably omits HMRC taxpayer data being in the plans outlined by the Sudlow Review. The mention on page 90 is so opaque you could be entirely forgiven for missing that your tax records are being linked to your health records and data mined in ways you have no awareness of (while academic projects are publicly disclosed, projects internal to government are kept secret as clubcard culture has taken over the “digital centre of government”).
The HMRC/health data linkage is not used to give or refuse care – it is a model used to say what types of treatments help economic growth (and so should be treated faster), and which don’t (and so people can wait longer), in general terms, for people like you.
Simultaneously, DH/E is centralising waiting list cleansing and prioritisation in Palantir means DH/E will be centrally setting the criteria for who gets the limited resource of an operating theatre or specialist care, replacing centrally what is currently done by the doctors in your hospital making decisions based on clinical need.
Like equivalent analysts at US health insurers, ONS will claim their findings don’t affect your care, but it is intended to affect the priorities of care provided to people like you for care you may need in future. If the care you need doesn’t promote economic growth then being rich won’t help you, and if you happen to have a disease of the rich then your poverty doesn’t matter. It’s all about “in general” not you specifically. But, diseases of London have a bigger impact on the economy than diseases of Blackpool or the North, so waiting lists in London should be prioritised according to the logic that the previous government used to start the NHS down this analysis path.
The Everyone Database: names, addresses, dates of birth, and all the identifiers used for you across Government linking all the data government has
I’ve previously sat in a UKRI meeting where a Professor spoke at length that he was not suggesting creating a population index or population register, while his slide behind him said he was, and he wanted it to be based on the NHS patient register. They had invited no one from the NHS to that meeting – they weren’t aware (until we told them). “Population Research UK” (another HDR sockpuppet) seems to have got them to do it anyway. If the meetings of that have started, has anyone from ONS noticed that everyone they’re talking to is basically Andrew Morris in a disguise?
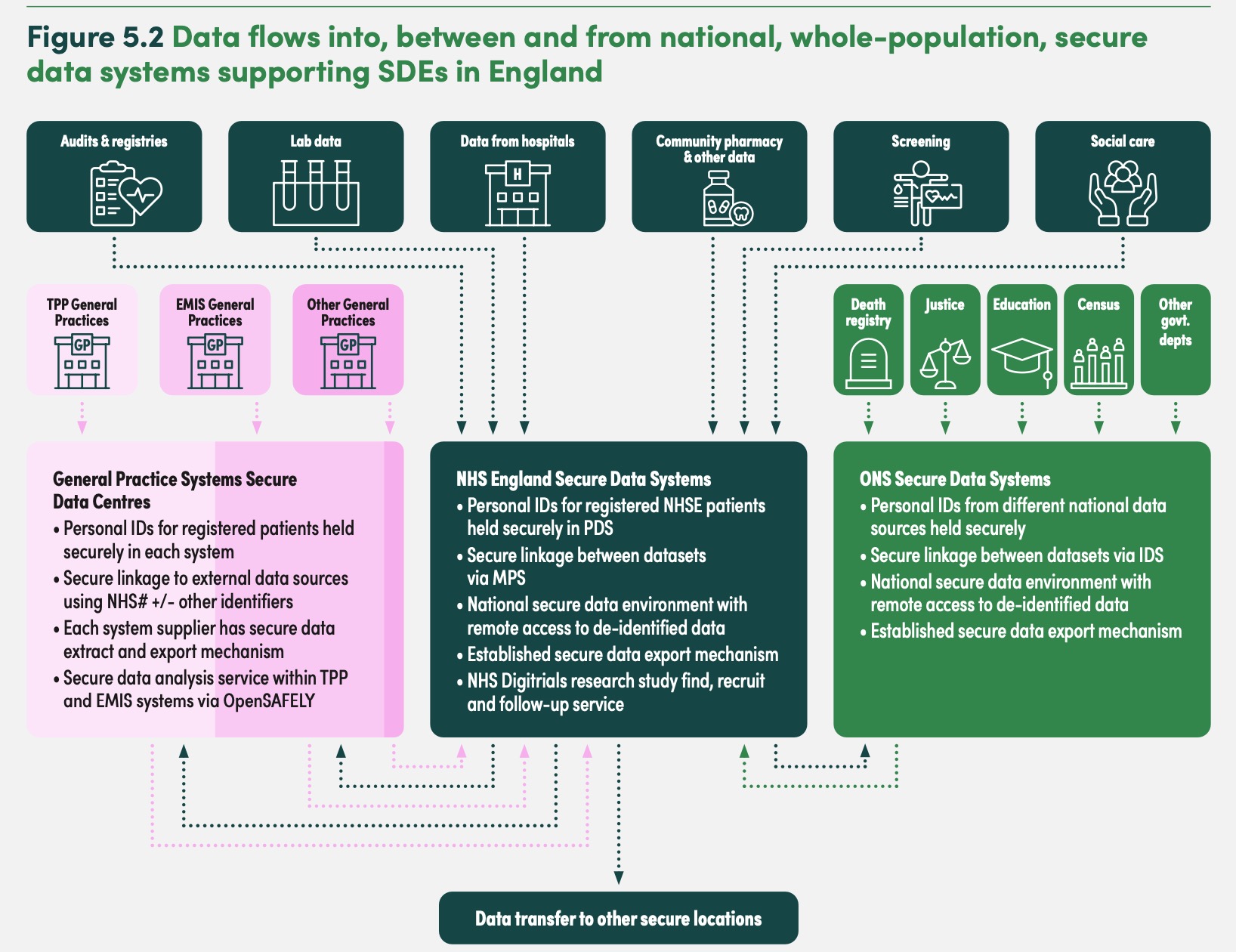
On page 123 the Review discloses what the Database is, and at the review launch, National Statistician Ian Diamond disclosed ONS had already built the “demographic index” and are using it as the link between tax and health records in order to do the analysis of which care to prioritise and which to deprioritise (ie cut).
The inclusion of justice data is particularly troubling – given it is a database of the victims of crime, not just perpetrators, mostly because HDR/Sudlow didn’t bother to think of those in any database as people with rights or concerns (or think of them as people at all).
The National Statistician has a choice

Speaking in 2021, Sir Ian Diamond, National Statistician said:
“There’s no god given right for us to have data. There needs to be a really sound public good reason for collecting data, and using data, and people need to feel absolutely comfortable that their data are being used properly and kept securely and in a way that satisfies all forms of privacy”
Does the National Statistician still believe that? If someone isn’t comfortable with that, for demonstrably good reasons, does the National Statistician want to use their data anyway? How does someone opt out?
At the HDR/Sudlow Review launch, he repeatedly talked about data being “used properly”.
Does “used properly” include the economic analyses that DH/E have announced being done on the data of people who have opted out of their data being used for purposes beyond direct care?
Does “used properly” include using the tax records of people who are given no choice about that at all?
As currently built, the ONS Population Index includes the NHS identifiers of everyone, but could easily have a second field which is only the NHS identifiers of people who have not got a national data opt out, and it is that second field which is used for research purposes. Until DSIT gives a “rest of government opt out” the “NHS national data opt out” is available, especially for NHS uses. The existence and scope for abuse of the Population Index is an entirely different problem (noting also that the spooks want access to everything any entity in the UK uses for anything). What happens when Home Office staff walk across the corridor from their open plan office into the ONS open plan office in the same building and want special access to data?
Some of the other simpler issues can resolve themselves – transparency will come to ONS either voluntarily or from outside. ONS can request a second dataset to which the National Data Opt Out has been respected, which is used for all research proposals (as AGD recommended); or as the HDR/Sudlow Review suggested for Biobank and the Department of Health in England, do promises only apply when it’s easier to keep them than not? Will ONS treat the census the same way?
ONS claims some abstract sense of “public support” for what they do, but they want data this way because public support for their work, in the very real measure of response rates to their flagship survey, is only 20% and falling. ONS claims of public support do not stand up against their own response rates.
==
(some of these issues came up at the UK Statistics Assembly on 22 January, where we were a discussant in a session)
For those who have followed medConfidential’s team since the 2000s, the institutional funders who focussed on these topics under the previous labour government seem to have moved on to other areas. We remain grateful for individual donations.
Pingback: A “national Digital ID system” – after the King’s Speech and HAC Report – NO2ID