The new “Ten Year Plan” shifts decision-making power from you and your family doctor to hospitals and technology companies. There are wordings from the political leadership about patients owning data, but the depths of the policy machine seems to suggest there be a day soon when you ask the NHS to opt your data out of being used for purposes other than you care, and it will do less than it does today.
Any plan is an exercise in tradeoffs, but leadership is about making and explaining those hard decisions. Mr Streeting did neither.
Critics of the pre-pandemic 2020 planning said the system had no real plan—barely even a plan to make a plan. The new plan is barely a plan to have a plan. Even the Blair Institute found it underwhelming. The tradeoffs needing leadership were ducked, epitomised by the complete absence of a “delivery” chapter.
It is delivery that matters for patients – 150 pages of irrelevance unless there is delivery.
New ideas are scarce – it largely rehashes previous plans, sprinkled with some AI ‘fairy dust’. But the fact that the Government has no idea how to deliver any of it means they at least don’t have to be talked out of an entrenched position, they can be steered out of their confusion by those working in the wider public interest (which will require listening to more than the hospitals and tech suppliers that confused things in the first place).
It is clear some decisions have been made:
1) Single Patient Record on Palantir’s Federated Data Platform
One of the pre-announcements was Palantir/FDP doing the maternity care monitoring, and the 10YP (page 48, bottom right) says that will be done with the data in the SPR – so Palantir will run the SPR with all data being owned by the politicians of the day, including full DNA sequences. Perhaps the incoherent “request for information” from a couple of months ago was the sham some suppliers suspected it was.
The political decision appears to have been made and withheld from the public, which does not bode well for public trust in the 10YP. As with the US, Palantir came first for babies.
As the 10YP says: “The NHS never has the right to keep the public in the dark. That it so often does so reflects the centralisation of power and disregard for patient voice we identified in chapter 5.”. NHS England has recently decided that more data projects can be hidden from the public (items 5.2, 5.3, 9).
If the “app first” AI led vision works, your NHS app doesn’t need a Single Patient Record at all, it can connect data from multiple places and display it all for you. Your device can run those algorithms and you can make an informed decision about prevention, rather than having all the data under the control of the Secretary of State for him to run his algorithms and tell you that you’re fat. The Dash Review on patient safety, written by the now-Chair of NHS England, remarkably doesn’t mention the Single Patient Record at all, talking of doing what it needs in the Federated Data Platform (using data would be in SPR if both weren’t in Palantir).
The only thing moving all your health records to Palantir uniquely adds is the ability for Mr Streeting – and his Reform successors – to run algorithms over your record to implement political decisions about your care. If the decisions were in your interests, your NHS app could run them locally for you.
2) Is your Politically Controlled Single Patient Record yours?
If you “own” your record, that’s good, but you have to actually have the power and control that come with owning something.
In most places in this Plan there is a lot of repeated text promising the same things over and over; but the section about the SPR being under patients’ control and patients being empowered is curiously not repeated in the same way the AI hype is. “Ownership will be with the NHS or patient” suggests that the patient isn’t in control when the NHS doesn’t want the patient to have a say.
You have no right to delete data from your official medical notes – even if it was a phase in your life long ago with temporary troubles, or a hallucinating AI summariser added some fiction about a consultation, once something has been added to your medical notes it is impossible to remove. It will be there, visible wherever the NHS logo is seen to any doctor who looks and read by any AI tasked to run.
Some exact quotes:
- (pg 11) “for the first time ever in the NHS, give patients real control over a single, secure and authoritative account of their data and single patient record to enable more co-ordinated, personalised and predictive care”
- (pg 11) “More fundamentally, we believe fast, transparent and secure access to our own health data is a right, not a privilege.”
- (p48) – We have spoken to the public around the country about how they want their data to be used. We heard their desire for a rigorous approach to privacy and security, which will inform our redesign of the opt-out system”
And then all the caveats appear:
- (p48) “We will reform the legal framework to allow for health data to be used to improve the NHS and for research that benefits its patients – including, through the Health Data Research Service announced by the Prime Minister in April 2025.”
- (p116) “Deidentified data will be made available to scientists”
- (p117) “We will work with the public as we develop the details on this, but for the avoidance of doubt, this will never mean compromising on patient privacy. Data ownership will remain with the NHS or patient.”
- (p117) “we will explore ways to derive commercial value from access to anonymous health data as well as from public assets like advanced analytics”
If patients do not want the data that they “own” to be used, then it should not be used.
In one place the Plan says patients will have “real control” over their record and “data ownership will remain with the NHS or patient”. The “or” implies that the NHS can continue to make decisions the patient objects to.
The contradictions and caveats in the 10YP suggested the current mess of loopholes is likely to continue, with opt outs being ignored two thirds of the time today. The only differences under the SPR will be much more data and there will be less scrutiny from the GP Profession with their obligations to you as a patient.
The work to “reform” the National Data Opt Out has been indistinguishable from push-polls encouraging patients to let NHS England do whatever it likes. With the abolition of NHS England, that will become the Department of Health in England, and the politicians in charge are deciding what they can do with your entire health record. And the answer seems to be anything they wish. The proposed legislation has to be water tight, and there is no track record of the hard decisions being made that will make it anything other than another dodge of responsibility.
Taken together, there is likely to be a day in 2026 when opting out will do less than opting out does today.
What Government does is as important as what Government says it should do.
3) (Lack of) delivery is political
The “delivery” chapter is entirely missing.
The plan assumes patients should only have the agency that the Secretary of State is willing to give them, and the plan entirely relies on the Secretary of State always having the interests of Wes Streeting and never the interests of Andrew Lansley.
The tech companies running digital services can impose changes on you and you can accept the new terms or not use the private service offered on a take it or leave it basis; with public services you have a view.
The plan puts the tech guys on top; mere patients will use apps and will like it. Patients must use 111 chatbot to get permission to visit A&E and will like it. Their GP practice site will be closed and move to a hospital managed neighbourhood health centre about as local as the job centre (there’ll be about the same number of both). These changes are good for hospitals and tech cos – the primary authors of the plan – but like all the long known good ideas, the hard bit is delivery. There is scope for new national digital services – a high quality digital service like SH:24 could easily be a national service, the barriers are all on policy and the choices of structures. The most obvious ban that is likely to be removed is cross selling commercial services to NHS patients who shouldn’t have to pay for any of them. Using the NHS app for your GP will become more like your NHS dentist where treatments are increasingly private.
It’s entirely rational for a hospital to want to manage their own front door, when they don’t have the ability to move people out of hospital and into social care at one end, they’ll feel the need to restrict access to A&E at the other. That it’s rational for the hospital to want it does not mean it is the only answer, or that it’s rational for the Secretary of State for Health and Social Care to say that is the policy he is going to deliver. But when you give more power to hospitals, what you get is more powerful hospitals wanting policies that make it easier to run hospitals.
There will be an election by 2029, and it will be a politically open goal for the opposition(s) to say “we’ll remove Wes Streeting’s ban on visiting A&E without an appointment”. And after Labour lose, your local neighbourhood health centre will go the way of your local sure start centre (but since it’ll be privately run, those in richer areas will stay for private patients only).
Wes can force everyone’s data into the Single Patient Record, he can pass legislation that lets him do whatever he likes, and micromanage your health using algorithms and sensors on your device. There is no commitment to all services remaining on the NHS.UK website that are available on the app, so those without the app can still access all services.
Much of the tension and challenge in projects comes from delivery choices. The vision was grand, the delivery is often something else. The plan has ignored all the delivery choices and promises little prior to 2035.
Innovation
“Ambient Voice Technologies” may sound like a harmless innovation until it’s reworded as microphones recording every consultation, and patients simply stop telling their doctors the sensitive truth. The AVT suppliers will get pressured by their lawyers to first include all transcripts in medical records, and then all audio recordings because safeguarding and safety.
Time moving forwards means we learn things, while the plan assumes Mr Streeting will learn nothing during the period; which may be true but it’s a damning indictment of the expectations set by politicians who want to be data controllers for your health record.
Politically it is difficult to rely on magic beans that do not yet exist. But the plan assumes that none of the money going into health research will deliver anything. The scope for vast quantities of budget to be freed up for innovation moving major treatments from hospital to GP and pharmacy is entirely missing. The plan contains limited recognition that any innovation other than AI will occur before 2035, and leaving hospitals in charge of everything will mean that delivery and innovation only happens in hospitals, while innovations outside hospitals are slowed.
It’s incoherent for the plan to assume that any AI the authors like will work perfectly in all cases, while nothing else will advance at all. CRUK pour money into curing cancer and the mRNA treatments show promise, Google DeepMind says their new drugs will be in testing this year, something might work by 2035, but there’s no certainty it will work but it would be astounding if nothing worked. The dementia charities have realised fraud put them on the wrong track and are now looking at new models of treatments; blood tests for everything are starting to offer some degree of delivery. If this plan was written 5 years ago today, we would not yet know whether the mRNA vaccines for covid worked in the way we do now. A plan written 10 years ago would have lauded social media for informing and engaging patients in communities, rather than addressing the new patients with new mental health needs. This part of the “plan” is not a plan.
Hospitals will do whatever they are resourced to do for particular conditions, GPs are the only part of the NHS that treats the whole patient and has a responsibility to you as a human not you as a condition. If GP loses influence over data, your data will be treated as a collection of interesting conditions more than data about you as a person. (this is the basis of the HDR unconsented cohorts project we’ll cover in future)
Delivery is possible
“It won’t be easy” says the Prime Minister in the introduction recognising the scale of what should follow, but wrapping up his plan Mr Streeting says “there are moments… when our choices define who we are” after dodging all of those choices.
The cowardice of cutting the delivery chapter shows how weak the plans are – there is no plan for delivery. But it does mean that the good bits of the plan can be moved forward, but companies will push forward the most profitable parts. The thinking of the Department of Health in England is that imposing passports everywhere will be the solution to everything; the Home Office and Blair Institute argue that doesn’t work.
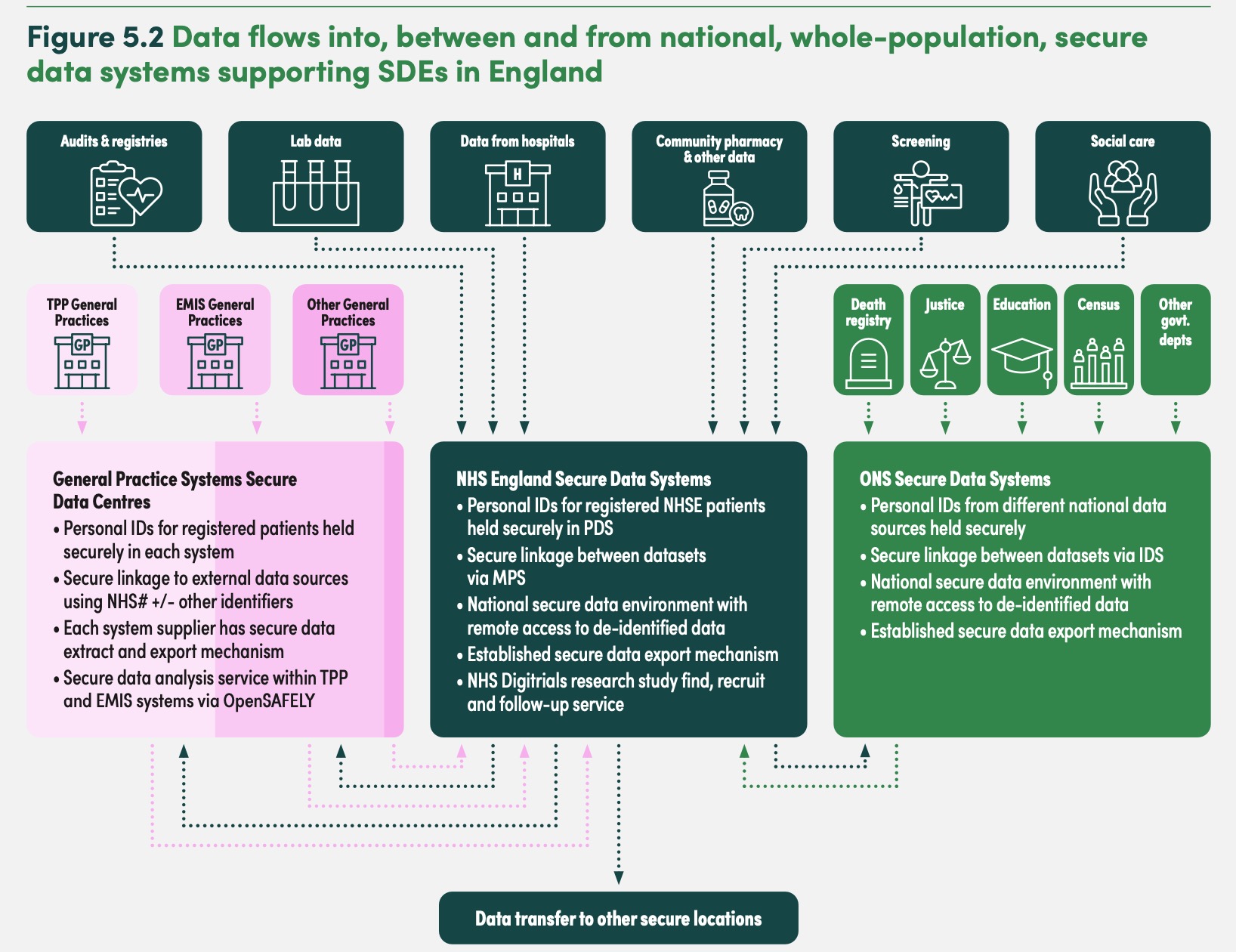
Over the next few weeks, we’ll look at how the policy intent can be delivered in ways that ensures that every flow of data into, across and out of the NHS and care system is consensual, safe, and transparent, showing there need be no conflict between good research, good ethics and good medical care.
===
In addition to our annual-ish newsletter, you can also join our free substack to get emailed whenever we post some news or commentary.